Practice Management | Revenue Cycle Management | Revenue & Finances | Financial Management
Over the past year, one topic has come up in nearly every conversation I’ve had with specialty practice professionals, executives, and revenue cycle leaders. Denials are up – in many specialties approaching 15%-20% – and for many organizations it feels like a constant effort just to keep pace.
Practice Management | Revenue Cycle Management | Revenue & Finances | Financial Management
Earlier this year at Nextech EDGE 2026, I had the opportunity to sit on a panel alongside several leaders deeply embedded in the realities of revenue cycle performance. These were not theoretical conversations. Each of us brought a perspective shaped by what we see inside organizations every day.
EHR | Technology & Innovation | Healthcare Technology
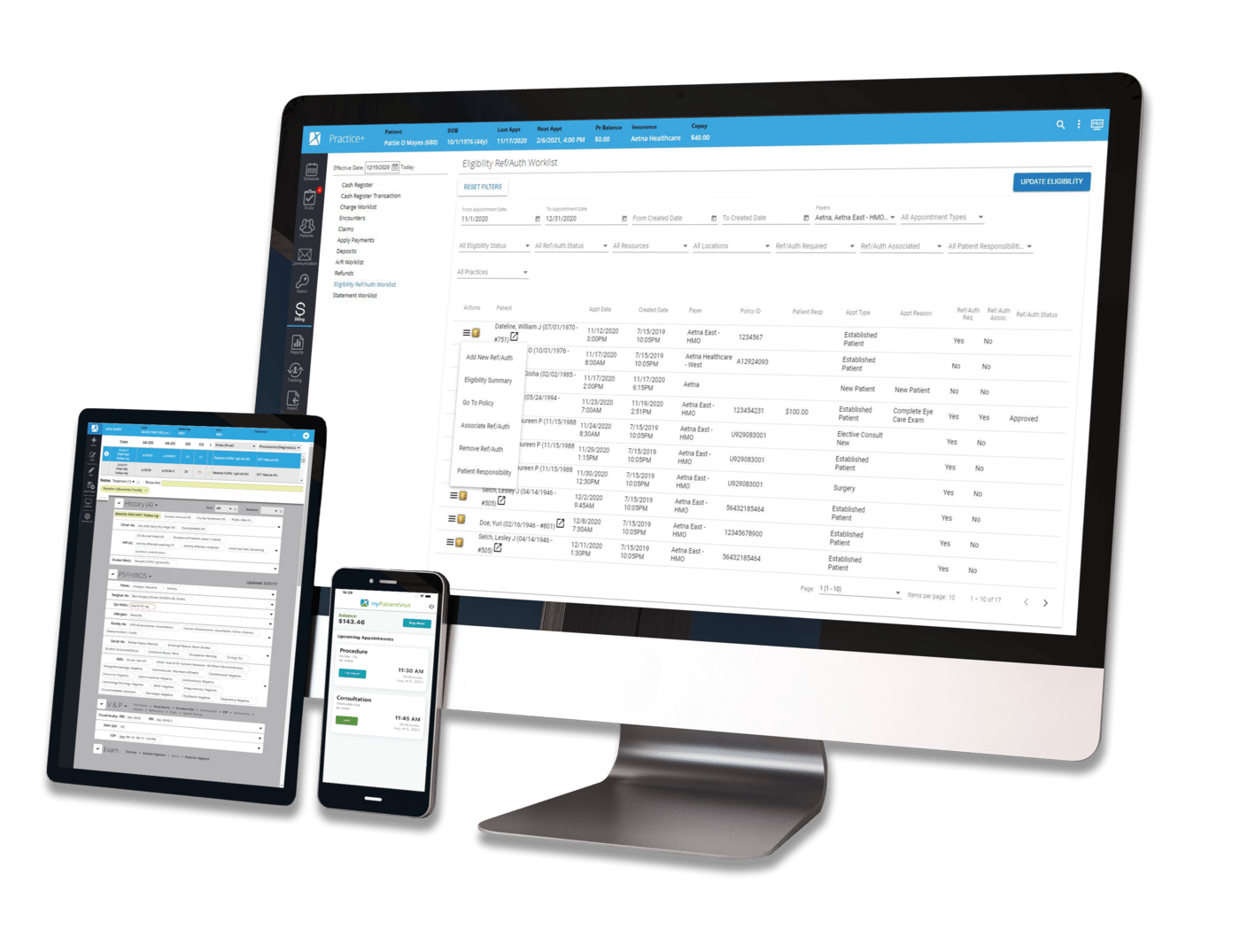
If your practice is still running on an on-site EHR, you’re not alone. But you may be falling behind. Across specialty healthcare, the pressure is building. Systems that once felt reliable are now slowing teams down, limiting visibility into performance, and making it harder to keep up with rising patient expectations and evolving compliance requirements. What used to work may now be creating friction at nearly every step — from documentation and scheduling to billing and reporting. A cloud-based EHR offers a fundamentally different approach. But for many practice leaders, two key questions remain: Will switching be worth it? How quickly can it be implemented? The benefits of cloud-based EHRs (short- and long-term) How security actually compares to on-premises systems Where ROI comes from and what you may be losing today A step-by-step roadmap to implementation In this guide, we’ll break down:
Plastic Surgery | Plastic Surgery Software | Technology & Innovation
There’s a moment every growing plastic surgery practice reaches with their technology — when what once worked, no longer does.
Government | Revenue Cycle Management | Regulatory & Compliance
I recently spent time on Capitol Hill as a provider representative in conversations about several exigent healthcare topics with leaders from the Centers for Medicare & Medicaid Services, members of Congress, staffers, and policy advisers. What struck me most was not disagreement. It was distance.
Ophthalmology | AI | Cora AI
Artificial intelligence (AI) is changing healthcare, yet it will never replace the experience, insight, and leadership of physicians. Still, AI is becoming clinically and operationally indispensable, especially in ophthalmology. It strengthens what physicians and their care teams do best: deliver precise diagnoses, personalized treatment, and meaningful patient care.
The medical aesthetics industry is growing at a rapid pace, and opening a med spa is more complex than ever.
cybersecurity | Regulatory & Compliance | Security & Data Management
Cyberattacks are a direct threat to patient safety, financial performance, and the day-to-day operations of your practice. A single breach can halt scheduling, delay procedures, expose sensitive patient data, and disrupt revenue for days or even weeks. The days of cybersecurity being only a back-office IT concern are over.